The Problem of Misdiagnosis in Hypermobility Spectrum Disorders
By Jennifer Richards, LMT
Hypermobility Spectrum Disorders (HSD) and hypermobile Ehlers-Danlos Syndrome (hEDS) are connective tissue disorders that frequently go unrecognized in clinical practice. Because connective tissue is present throughout the body, symptoms often involve multiple organ systems. When these symptoms are evaluated in isolation, patients may receive incomplete or incorrect diagnoses.
The result is not simply delay — but sometimes treatment that worsens instability or fails to address the underlying mechanism.
Why Hypermobility Is Commonly Missed
hEDS is currently the only Ehlers-Danlos subtype without a confirmed genetic marker. Diagnosis is clinical and based on criteria established in the 2017 International Classification of the Ehlers-Danlos Syndromes.
HSD is diagnosed when symptomatic joint hypermobility is present but full hEDS criteria are not met.
Because there is no single laboratory test to confirm hEDS/HSD, diagnosis requires:
A detailed history Beighton score assessment Evaluation of systemic features Exclusion of alternative diagnoses
Unfortunately, many providers are not trained to recognize the multisystem patterns associated with connective tissue disorders.
Frequently Reported Misdiagnoses
Below are conditions commonly diagnosed in patients later found to have HSD or hEDS. In some cases, these diagnoses may coexist. In others, they represent diagnostic overshadowing.
1. Systemic Lupus Erythematosus (SLE)
Patients with hypermobility frequently present with:
Joint pain
Fatigue Raynaud’s phenomenon
Rashes
Non-specific systemic complaints
These symptoms often prompt an autoimmune workup.
The antinuclear antibody (ANA) test is typically the first screening tool for lupus and related connective tissue diseases.
Research indicates:
A negative ANA has high negative predictive value for SLE. Over 95% of lupus patients are ANA positive.
When ANA testing is negative and other autoimmune markers are absent, clinicians may conclude that systemic autoimmune disease is unlikely.
However, the absence of autoimmune markers does not explain:
Mechanical joint instability
Recurrent sprains/subluxations
Orthostatic intolerance
GI dysmotility
In such cases, hypermobility should be considered.
Why Mislabeling Matters
If autoimmune disease is presumed:
Immunosuppressive agents Corticosteroids Biologics
may be prescribed.
Long-term corticosteroid use is known to weaken connective tissue, reduce collagen integrity, and increase risk of tendon injury — potentially worsening symptoms in individuals with underlying connective tissue fragility.
2. Sjögren’s Syndrome
Sjögren’s is characterized by:
Dry eyes
Dry mouth
Fatigue
Joint pain
Interestingly, individuals with dysautonomia — particularly those with small fiber neuropathy — may also experience dryness due to autonomic dysfunction affecting glandular secretion.
Additionally:
Dysautonomia can impair lacrimal and salivary gland regulation. Small fiber neuropathy has been documented in both Sjögren’s and hEDS populations.
When SSA/SSB antibodies are negative and biopsy findings are absent, Sjögren’s may be excluded — yet symptoms remain.
The autonomic component of hypermobility is often overlooked in this differential.
3. Fibromyalgia
Fibromyalgia and hypermobility frequently overlap.
Research suggests a significant percentage of individuals diagnosed with fibromyalgia demonstrate generalized joint hypermobility.
However:
Fibromyalgia is characterized by central sensitization. Hypermobility includes structural joint instability.
If mechanical instability is not addressed through targeted stabilization and neuromuscular control, symptoms may persist despite standard fibromyalgia treatments.
4. Anxiety and Panic Disorder
Dysautonomia — particularly Postural Orthostatic Tachycardia Syndrome (POTS) — is strongly associated with hypermobility.
Studies estimate that a substantial percentage of individuals with POTS meet criteria for hypermobility disorders.
Symptoms of dysautonomia include:
Tachycardia
Lightheadedness
Tremulousness
Shortness of breath
Sweating Exercise intolerance
These can mimic panic disorder.
While anxiety may coexist, autonomic dysfunction is physiologic. Failure to perform orthostatic vitals or tilt-table testing may lead to psychiatric mislabeling.
This has consequences:
Delayed autonomic treatment Inappropriate medication choices Psychological invalidation
5. Irritable Bowel Syndrome (IBS)
Gastrointestinal involvement in hypermobility may include:
Delayed gastric emptying
Esophageal dysmotility
Constipation
Diarrhea
Visceral hypersensitivity
Connective tissue abnormalities affect smooth muscle support and enteric nervous system regulation.
IBS may be diagnosed appropriately — but without recognition of underlying connective tissue laxity, management strategies remain incomplete.
6. Early Degenerative Joint Disease
Because hypermobile joints experience increased shear forces and microinstability, early degenerative changes may occur.
Patients are sometimes told:
“You’re just wearing out early.” “It’s early arthritis.”
While degeneration may be present, the biomechanical cause — instability — may not be addressed.
Dysautonomia: A Critical Missing Piece
Autonomic dysfunction is one of the most underrecognized aspects of hypermobility.
Mechanisms proposed in the literature include:
Vascular connective tissue laxity leading to venous pooling Impaired vasoconstriction
Small fiber neuropathy
Abnormal baroreceptor signaling
Symptoms may include:
Orthostatic tachycardia
Temperature intolerance
Exercise intolerance
Brain fog
GI dysmotility
Urinary dysfunction
Without recognition of dysautonomia, patients may undergo years of fragmented evaluations.
What If the ANA Is Negative?
A negative ANA:
Significantly lowers likelihood of systemic lupus. Does not rule out hypermobility. Does not explain persistent mechanical instability.
If symptoms include:
Recurrent sprains
Joint hyperextension
Chronic “tight” muscles despite flexibility
Orthostatic intolerance
GI dysmotility
Family history of hypermobility
Further evaluation for HSD/hEDS may be warranted.
Suggested next steps:
Beighton score assessment
Review of 2017 hEDS criteria
Orthostatic vitals
Referral to providers familiar with connective tissue disorders
The Risk of Incorrect Treatment
Misdiagnosis may lead to:
High-velocity manipulations in unstable joints Aggressive stretching protocols Long-term corticosteroid exposure Unnecessary psychiatric labeling Surgical interventions without addressing instability
In hypermobility, stability — not increased range — is typically the therapeutic priority.
Why Proper Diagnosis Matters
Accurate diagnosis allows for:
Targeted stabilization strategies Autonomic support protocols Energy management education Multidisciplinary coordination Patient validation
It reframes the narrative from “medically unexplained” to “mechanically and neurologically complex.”
Closing Thoughts
Hypermobility is not rare.
It is underrecognized.
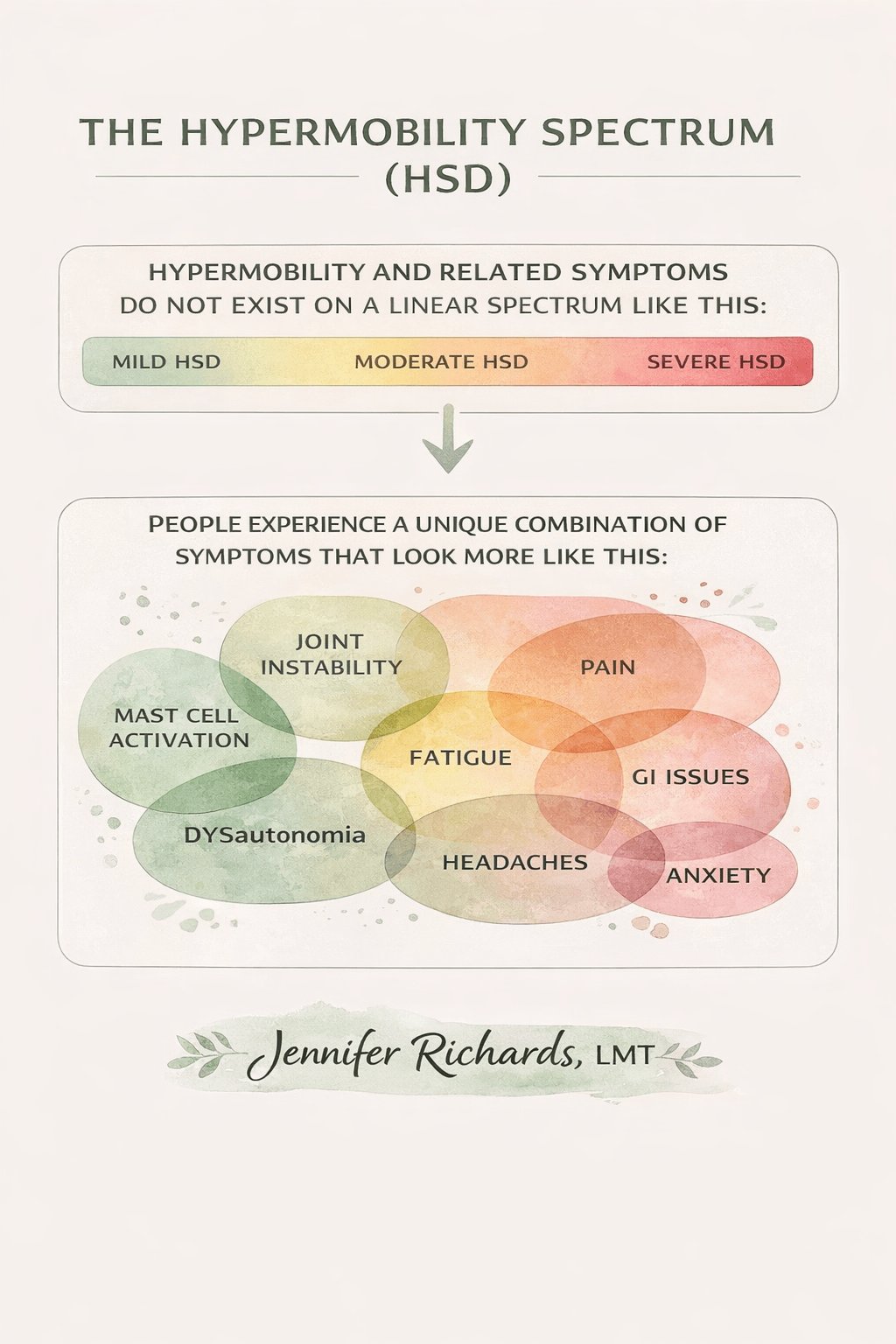
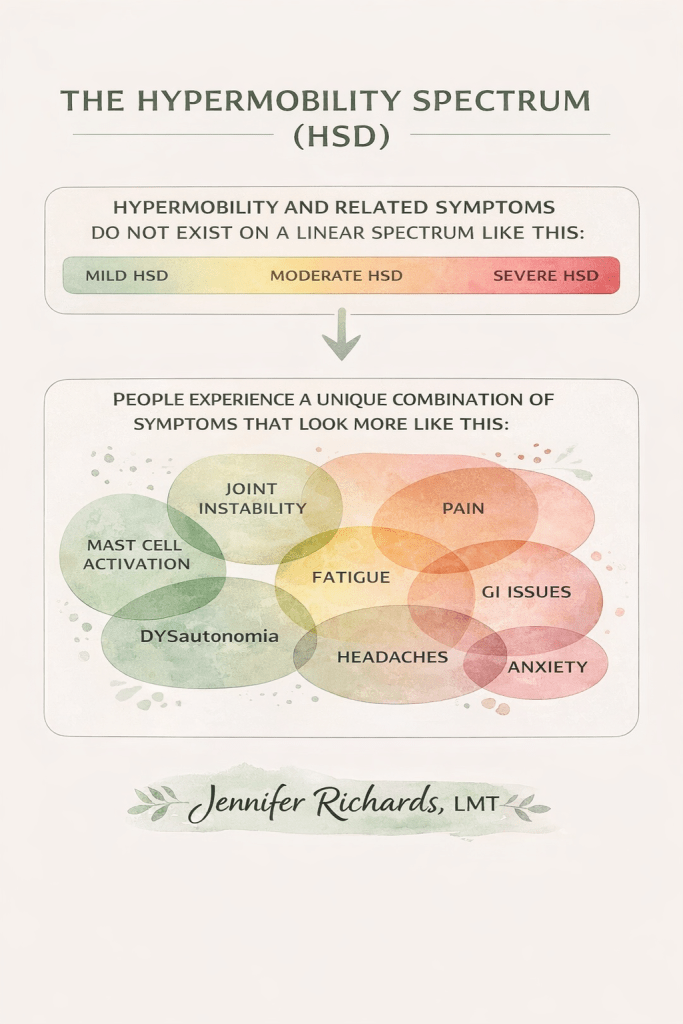
The spectrum is not linear, and symptoms do not always fit neatly within one specialty.
When autoimmune panels are negative and symptoms persist, connective tissue should be considered.
A correct diagnosis does not erase symptoms — but it changes the strategy.
And strategy matters.
Disclaimer
This article is for educational and informational purposes only and does not constitute medical advice. Diagnosis and treatment decisions should be made in consultation with qualified healthcare professionals. If you suspect a connective tissue disorder or autonomic dysfunction, speak with your physician or a specialist experienced in hypermobility spectrum disorders.
